Endometriosis is common; about one in ten women will develop it, yet staging still causes confusion. I regularly see patients who were told they have “minimal” disease and feel anything but minimal. I also operate on women with advanced scarring who were unaware of how extensive it had become.
The stage reflects how much disease is present anatomically. It does not measure how much it hurts.
HOW STAGING IS DETERMINED?
The system most surgeons use is the revised American Society for Reproductive Medicine classification. During laparoscopy, we assign points based on the number of implants, how deeply they invade, whether adhesions are present, and whether the ovaries are involved.
That scoring places the disease into Stage 1 through Stage 4.
This classification is surgical. It cannot be confirmed by symptoms alone, and early disease is often invisible on imaging.
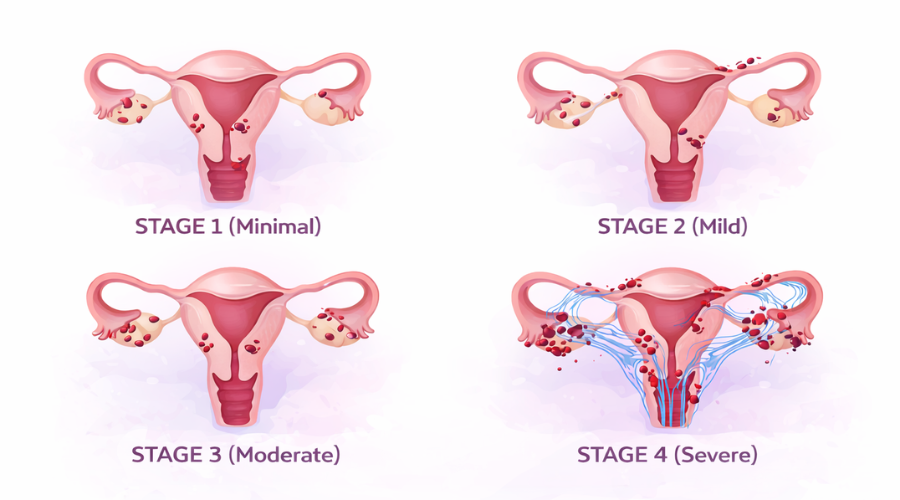
Stage 1 (Minimal)
Stage 1 usually consists of small, superficial implants scattered along the pelvic lining. There is little or no scar tissue. The anatomy remains largely undistorted.
This is the stage most likely to be dismissed. Imaging is often normal. Patients are told their pain is hormonal or functional.
Yet I have seen Stage 1 lesions sitting directly over sensitive nerve pathways that produce significant pain. Location matters more than surface area.
Stage 2 (Mild)
Stage 2 reflects a greater number of implants and slightly deeper invasion. Mild adhesions may begin to form, though the pelvic organs are still mobile.
Pain often becomes less predictable at this point. It may extend beyond menstruation. Intercourse may become uncomfortable. Patients sometimes describe a heaviness or pressure rather than cramping alone.
Although categorized as “mild,” symptoms are not necessarily mild.
Stage 3 (Moderate)
By Stage 3, scar tissue becomes more substantial. The ovaries may adhere to the pelvic sidewall or uterus. Endometriomas, blood-filled ovarian cysts, are common.
This is often the stage where fertility questions emerge. The fallopian tubes may be tethered. The ovaries may not move freely.
Chronic pelvic pain becomes more common, but again, the degree varies widely from patient to patient.
Stage 4 (Severe)
Stage 4 involves dense adhesions and deep implants. Organs may become fused together, sometimes creating what surgeons refer to as a “frozen pelvis.”
The bowel or bladder can be involved. Dissection becomes technically demanding. These are the cases where surgical experience matters most.
Interestingly, I have operated on Stage 4 patients whose primary complaint was infertility rather than pain.
RELATED: Endometriosis Vs Menstrual Cramps: What’s The Difference?
WHY STAGE DOES NOT EQUAL PAIN
Pain is influenced by depth of infiltration, nerve involvement, inflammation, and individual pain processing. A small implant infiltrating near a uterosacral nerve can produce disproportionate symptoms. Meanwhile, broad superficial disease may be less symptomatic.
This is why staging is helpful for surgical planning and fertility counseling, but limited in predicting suffering.
TREATMENT CONSIDERATIONS
Management depends on symptoms, age, reproductive goals, and disease distribution. Hormonal suppression can reduce the stimulation of implants. Surgical excision removes visible disease and releases adhesions. In women seeking pregnancy, preserving ovarian reserve is critical.
Each plan has to be individualized. There is no single algorithm that applies to every stage.
WHEN TO SEEK EVALUATION
Severe menstrual pain, pain with intercourse, bowel or bladder pain during cycles, or unexplained infertility warrant proper evaluation. These symptoms are not simply part of being a woman.
For more than three decades, I have treated women with complex pelvic pain and endometriosis in Los Angeles and Glendale. Staging helps determine what must be addressed surgically and what should be monitored long-term.
If your symptoms have been minimized or your diagnosis feels incomplete, a thorough consultation can clarify the situation and outline appropriate next steps.