Severe pelvic organ prolapse can significantly affect a woman’s day-to-day life, from exercise, intercourse, urinary and bowel function, to body image. Once they look for a solution, many have been told that a hysterectomy is the only solution. In many cases, that simply isn’t true.
In my practice, I focus on restoring normal pelvic support while preserving function and, when appropriate, preserving the uterus. Over time, I’ve developed a vaginal, minimally invasive approach that allows me to correct even advanced prolapse without removing the uterus, with reliable and durable results.
UNDERSTANDING SEVERE PROLAPSE
Pelvic organ prolapse is typically a combination of defects rather than a single issue. Most patients present with:
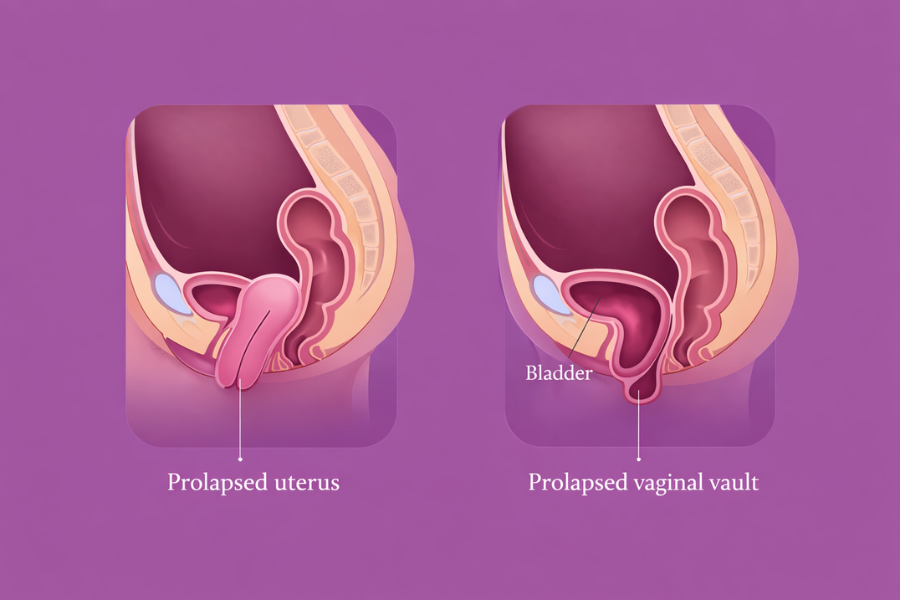
- Loss of apical support (uterine descent)
- Anterior vaginal wall weakness (cystocele)
- Posterior vaginal wall defects (rectocele or enterocele)
Similar to the four walls in a room, addressing only one vaginal wall often leads to recurrence. A successful repair requires identifying and correcting each level of support.
WHY I PRESERVE THE UTERUS
The uterus itself is not the cause of prolapse. The underlying issue is failure of the supporting ligaments and connective tissue.
I often see patients who previously underwent a hysterectomy and later developed vaginal vault prolapse. Removing the uterus does not correct the underlying support problem.
In appropriately selected patients, preserving the uterus allows for restoration of normal anatomy without removing an organ unnecessarily. It also maintains native support relationships within the pelvis.
VAGINAL RETROPERITONEAL MCCALL CULDOPLASTY
A key part of my approach is a modified vaginal retroperitoneal McCall culdoplasty, adapted to suspend the uterus. I began using this little-used technique many years ago in patients who medically were not able to tolerate a long surgical procedure requiring the removal of the uterus, and soon adapted the procedure to help those who did not want their uterus removed.
Using a vaginal approach, I access the uterosacral ligaments through the retroperitoneal space and use them as suspension points. Sutures are placed to elevate the uterus back into its natural position, and the cul-de-sac is closed to reduce the risk of enterocele.
This provides strong apical support without the need for abdominal surgery or mesh.
VAGINAL RECONSTRUCTION
In the same operation, I address the anterior and posterior vaginal walls based on each patient’s specific defects.
Anterior repair focuses on restoring the pubocervical fascia to support the bladder. Care is taken to avoid overcorrection.
Posterior repair involves reconstruction of the rectovaginal fascia and, when needed, the perineal body. This improves both support and function.
Each repair is tailored to the individual. There is no standardized template that works for everyone.
WHY THE VAGINAL APPROACH
Whenever possible, I prefer a vaginal approach. It allows direct access to the defects and avoids abdominal incisions. Patients typically experience less pain and a smoother recovery compared to abdominal procedures.
In most cases, this approach also allows me to avoid the use of synthetic mesh or, in some cases, address urinary incontinence issues at the same time.
RELATED: Urinary Incontinence and Vaginal Prolapse After Vaginal Delivery
OUTPATIENT SURGERY AND RECOVERY
A significant portion of these procedures can be performed on an outpatient basis. Many patients go home the same day.
Recovery is generally straightforward. Most patients are up and walking within a day, and activity gradually increases over the following weeks. Avoiding abdominal surgery plays a large role in this.
OUTCOMES
The goal is not just anatomical correction, but meaningful improvement in quality of life. Vaginal repairs have been shown to have high success rates and patient satisfaction.
Durable outcomes depend on proper identification of all defects, solid apical support, and a balanced reconstruction that preserves function. When these principles are followed, patients tend to do very well.
FINAL THOUGHTS
Pelvic organ prolapse is a support problem, not a uterine problem. In many cases, it can be corrected without removing the uterus.
A well-executed vaginal repair using retroperitoneal McCall culdoplasty, combined with anterior and posterior reconstruction, can restore support in a durable and minimally invasive way.
If you have prolapse that is affecting your quality of life or if you’ve been advised to undergo a hysterectomy and want a second opinion about preserving your uterus, you should know that other options exist. Contact us to book a consultation.